
Navigation: Assets → Accidents
Click here for information on how to use a data entry window
Accident ID and Status

|
Field |
Description |
|
Accident Id |
Search for an existing accident by entering the exact ID or using the lookup tool. A new accident record can also be created from this field. |
|
Status |
Select the current stage of the accident. |
Main - Primary Info
|
Field |
Description |
|
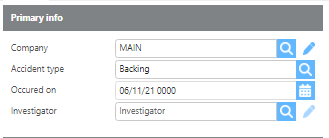
Company |
Select which company the accident occurred under. |
|
Accident type |
Select the appropriate accident type from the directory. |
|
Occurred on |
Enter the date and time the accident occurred. |
|
Investigator |
Select the user who is primarily responsible for handling this accident. |
Main - Address

|
Field |
Description |
|
Company name |
Enter the name of the company or location where the accident occurred. |
|
Address |
Enter the address where the accident occurred. |
Main - Accident
|
Field |
Description |
|
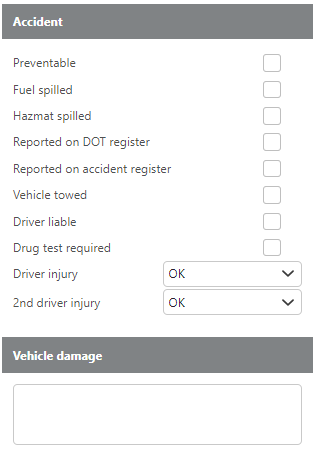
Preventable |
Check if the accident was preventable. |
|
Fuel spilled |
Check if fuel was spilled. |
|
Hazmat spilled |
Check if hazardous materials were spilled. |
|
Reported on DOT register |
Check if this accident should be reported on the DOT registry. |
|
Reported on Accident register |
Check if this accident should be reported on the Accident registry. |
|
Vehicle towed |
Check if the vehicle was towed. |
|
Driver liable |
Check if the driver is liable for the accident. |
|
Drug test required |
Check if a drug test is required as a result of this accident. |
|
Driver injury |
Check if the primary driver was injured. |
|
2nd driver injury |
Check if the secondary driver was injured. |
|
Vehicle damage |
Enter a description of any vehicle damage. |
Accident description
|
Field |
Description |
|
Accident description |
Enter a full description of the accident. |
Trip information - Primary Info
|
Field |
Description |
|
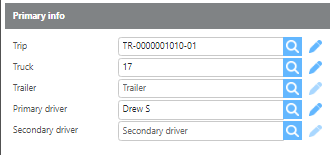
Trip |
If the accident occurred while the driver was on a trip, select it here. Selecting a trip will auto-fill the Truck, Trailer, Primary Driver, and Secondary Driver fields below. |
|
Truck |
Enter the truck involved in the accident. Auto-filled if a trip is selected. |
|
Trailer |
Enter the trailer involved in the accident. Auto-filled if a trip is selected. |
|
Primary driver |
Enter the primary driver involved in the accident. Auto-filled if a trip is selected. |
|
Secondary driver |
Enter the secondary driver involved in the accident. Auto-filled if a trip is selected. |
Trip information - Shipper
|
Field |
Description |
|
Company name |
Enter the shipper's company name. Auto-filled if a trip is selected. |
|
Address |
Enter the shipper's address. Auto-filled if a trip is selected. |
Trip information - Road conditions
|
Field |
Description |
|
Road conditions |
Enter any relevant road condition information at the time of the accident. |
Trip information - Consignee
|
Field |
Description |
|
Company name |
Enter the consignee's company name. Auto-filled if a trip is selected. |
|
Address |
Enter the consignee's address. Auto-filled if a trip is selected. |
Other party - Vehicle information
|
Field |
Description |
|
Make |
Enter the make of the other party's vehicle. |
|
Model |
Enter the model of the other party's vehicle. |
|
Make year |
Enter the year of the other party's vehicle. |
|
Color |
Enter the color of the other party's vehicle. |
|
Plate number |
Enter the license plate number of the other party's vehicle. |
|
Damage |
Describe any damage to the other party's vehicle. |
|
Fatality count |
Enter the number of fatalities, if any. |
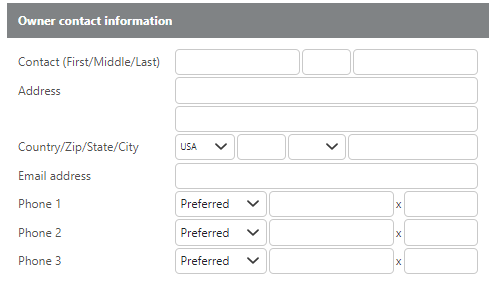
Other party - Owner contact information
|
Field |
Description |
|
Contact |
Enter the vehicle owner's name. |
|
Address |
Enter the vehicle owner's address. |
|
Email address |
Enter the vehicle owner's email address. |
|
Phone number |
Enter the vehicle owner's phone number. |
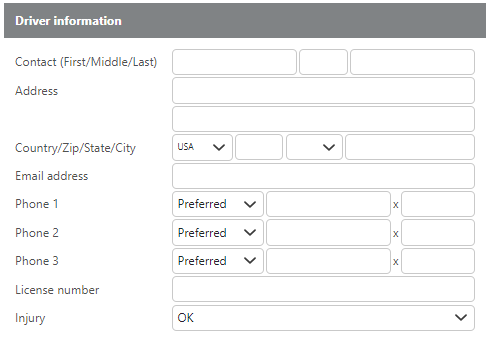
Other party - Driver information
|
Field |
Description |
|
Contact |
Enter the other party driver's name. |
|
Address |
Enter the other party driver's address. |
|
Email address |
Enter the other party driver's email address. |
|
Phone number |
Enter the other party driver's phone number. |
|
License number |
Enter the other party driver's license number. |
|
Injury |
Select whether the other party driver was OK, Injured, or if there was a Fatality. |
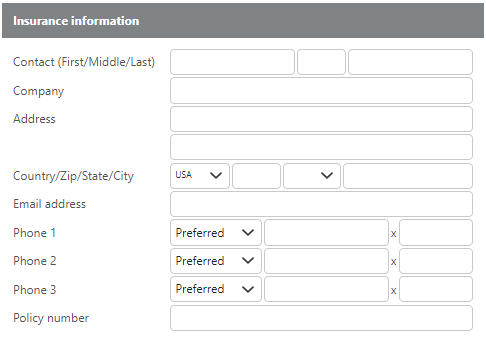
Other party - Insurance information
|
Field |
Description |
|
Contact |
Enter the insurance contact's name. |
|
Company |
Enter the insurance company name. |
|
Address |
Enter the insurance company's address. |
|
Email address |
Enter the insurance contact's email address. |
|
Phone number |
Enter the insurance contact's phone number. |
|
Policy number |
Enter the insurance policy number. |
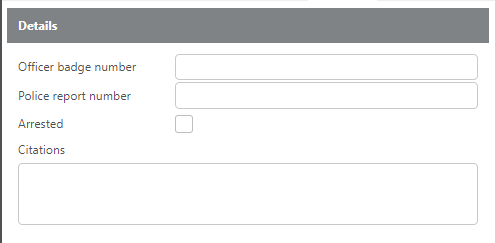
Police- Details
|
Field |
Description |
|
Officer badge number |
Enter the responding officer's badge number. |
|
Police report number |
Enter the police report number. |
|
Arrested |
Check this box if the driver was arrested |
|
Citations |
Enter the details of any citations issued. |
Claims
|
Field |
Description |
|
Add claim |
Click to link an existing claim from the Claims module to this accident. |
|
Create new claim |
Click to create a new claim directly from this accident record. This will open a new claim in the Claims module. |
Accidents Video